EHR Implementation Cost Breakdown: Critical Factors to Consider
Updated 04 Jul 2026
18 Min
133 Views
An EHR system sits at the center of nearly every clinical and administrative workflow in a healthcare practice, which means its cost is rarely just about software. The number you commit to shapes hiring, infrastructure, and how quickly your clinic recovers the investment. Most public price ranges leave clinic owners more confused than informed.
As an IT provider with 15+ years of experience building HIPAA-compliant software for clinics, hospitals, and digital health startups across the US and EU, we, at Cleveroad, see exactly where EHR projects go over budget and where they pay back. This guide breaks the price down, using internal benchmarks from our own delivery data rather than generic market averages.
Key takeaways:
- Off-the-shelf / SaaS adoption costs vary by clinic size: small practice $3,000–$25,000, mid-size clinic $25,000–$150,000, hospital $150,000–$1,000,000+.
- Custom EHR build: focused build $30,000–$80,000; mid-size clinic $60,000–$255,000 core development; hospital or enterprise $250,000–$1,000,000+.
- Four cost drivers move the EHR implementation cost the most: module scope, integration count, deployment model, and compliance scope.
Read on for the module-level breakdown, the hidden cost lines that overrun budgets, and the build-versus-buy math for a 15-provider clinic.
How Much Does EHR Implementation Cost?
EHR pricing splits into two paths. With SaaS adoption, you pay a license plus per-provider fees on a subscription, with little upfront spend. With custom development, you commission a product that the clinic owns. The same 15-provider clinic on either path can see a five-year total that differs by tens of thousands of dollars.
The table below compares published cost ranges by facility size on both paths.
| Facility size | SaaS / off-the-shelf adoption | Custom development |
|---|---|---|
Small / solo practice (1–5 providers) | $3,000–$25,000 | From $30,000–$80,000 (focused build) |
Mid-size clinic (10–50 providers) | $25,000–$150,000 | $60,000–$255,000 (core development) |
Hospital / large health system (100+ providers) | $150,000–$1,000,000+ | $250,000–$1,000,000+ |
Methodology: Ranges derived from Cleveroad’s healthcare delivery benchmarks at a $50–$80/hr development rate, cross-checked with public SaaS pricing pages and Clutch healthcare vendor profiles for 2025–2026.
Small and solo practices
A 1–5 provider practice sits at the bottom of the cost curve. On a SaaS plan, the all-in spend lands at $3,000–$25,000 with per-provider fees of $100–$600 per month. A focused custom build starts around $30,000–$80,000 and covers the essentials: patient records, scheduling, and basic billing.
The price moves up the moment you add integrations. A plan with no lab feed, no e-prescriptions, and no paper-record migration sits near the floor. Add one lab integration plus migration of three years of paper charts, and you approach the ceiling of the SaaS range.
Mid-size clinics and group practices
For a clinic with 10–50 providers, SaaS adoption typically runs $25,000–$150,000 and custom development covers $60,000–$255,000 for core development. License count, data migration volume, and the number of integrated systems explain most of the variance.
A clinic running on three or four disconnected SaaS tools that wants them unified often crosses the breakeven into custom builds faster than expected. The cost of duplicate license fees plus the time staff loses jumping between systems compounds quickly across a five-year horizon.
Hospitals and large health systems
Hospital deployments run $150,000–$1,000,000+, with no clean ceiling. The work is open-ended because it involves multi-department integration, enterprise platform licensing, and 12–24 months of implementation, which itself becomes a cost factor due to change management and clinical staff training time.
For a 200-bed hospital adding an EHR, the project typically spans at least two fiscal years. It involves interfaces with the lab information system, radiology PACS, pharmacy, billing clearinghouse, and at least one specialist registry. Each interface adds its own scoping cycle, contract, and test period.
Need a custom EHR built around your clinic’s workflows? Explore our EHR/EMR and patient portal development services to see how Cleveroad scopes and delivers healthcare platforms.
Why Does EHR Implementation Cost Vary So Widely?
Published ranges for EHR implementation costs span two orders of magnitude because four variables significantly affect the budget: deployment model, module scope, integration complexity, and compliance scope. Of these, integration complexity is the most consistent driver of budget movement in our delivery history. A clinic with three legacy systems often spends more on connecting them than on building any single new module.
Cloud vs. on-premise deployment
Cloud hosting pushes upfront cost down and operating cost up. On-premise inverts that ratio. An on-premise setup runs $50,000–$200,000+ upfront for hardware and infrastructure, with lower ongoing cost afterward. Cloud costs $100–$600 per provider per month with minimal upfront spend.
For a 15-provider clinic over five years, cloud costs roughly $300 × 15 × 60 months = $270,000. On-premises costs roughly $120,000 upfront plus about $15,000 per year, for a total of about $195,000. The crossover happens around year 3–4, and on-premise wins on cost only when the clinic already has an IT team to maintain it.
The table below summarizes the trade-off across upfront, recurring, and operational factors.
| Factor | Cloud | On-premise |
|---|---|---|
Upfront cost | Minimal | $50,000–$200,000+ |
Recurring cost | $100–$600 per provider/month | About $15,000/year for upkeep |
Five-year total (15-provider clinic) | About $270,000 | About $195,000 |
IT team requirement | Light | Heavy — needs dedicated IT staff |
Best for | Clinics with no dedicated IT team | Hospitals with internal IT capacity |
Methodology: Calculated at the cost ranges published above, using a 15-provider mid-size clinic baseline. Excludes one-time data migration and training; those are itemized separately in the Hidden Costs section.
Number of modules and user roles
Module count is the second biggest driver after integration. Cost tracks the feature set and role complexity more than headcount alone. A 50-provider clinic that needs only patient records and scheduling spends less than a 10-provider clinic that needs records, scheduling, billing, telehealth, e-prescriptions, and a patient portal.
Each user role you add (admin, provider, patient, billing, lab tech) brings its own access control rules and interface to design and test. Roles compound; they do not stack linearly. This sets up the module-by-module breakdown later in the article.
Integration count and complexity
Integration cost falls into three tiers: simple, medium, and complex. The table below shows typical effort, cost, and example systems for each tier.
| ntegration type | Effort (h) | Cost at $50–$80/hr | Example systems |
|---|---|---|---|
Simple (standard API) | 80-190 hours | $4,000-$15,000 | Basic webhooks, single REST endpoint |
Medium (practice management or telehealth) | 200-500 hours | $10,000-$40,000 | DoseSpot for e-prescribing, Vonage for telehealth video |
Complex (HL7/FHIR or legacy hospital systems) | 500-1,250 hours | $25,000-$100,000+ | Lab information systems, hospital LIS, legacy mainframe interfaces |
Methodology: Effort estimates drawn from Cleveroad’s healthcare integration work between 2023 and 2025, including DoseSpot, Surescripts, and HL7-based lab feeds.
The integration targets that come up most often in our healthcare projects: DoseSpot or Surescripts for e-prescriptions, lab and LIS systems for results delivery, and billing clearinghouses such as Change Healthcare or Availity. Each of these falls into the medium or complex tier, which is why integration is the single biggest budget mover in mid-size and hospital EHR builds.
Compliance scope by region
HIPAA compliance adds roughly 15–40% to a US EHR project, but the percentage hides what the work actually involves. Replacing that vague multiplier with itemized engineering lines makes the budget defensible.
Itemized HIPAA compliance engineering (total $14,500–$60,000, 290–750 h):
- Audit logging and access trails: $3,000–$12,000 (60–150 h)
- Encryption at rest and in transit: $2,000–$9,600 (40–120 h)
- Role-based access control: $4,000–$16,000 (80–200 h)
- Business Associate Agreement handling and vendor review: $1,500–$6,400 (30–80 h)
- Penetration testing and security audit: $4,000–$16,000 per cycle (80–200 h)
With 15+ years in custom HealthTech software development, Cleveroad builds medical solutions that keep patient data protected and consultations compliant. For Codex Labs, a Silicon Valley plant-biotechnology company, our team stabilized and delivered DECODE.ME, a teledermatology platform. We inherited an unstable codebase and made it HIPAA-ready: a full system assessment and code review, critical bug fixes, and secure infrastructure for virtual doctor–patient consultations, with encrypted PHI and audit-ready access controls.
See how Barbara Paldus, Founder and CEO of Codex Labs, describes the cooperation, and why she recommends Cleveroad as a reliable HealthTech development partner.
Dr. Barbara Paldus, CEO at Codex Labs: Feedback on Cleveroad's Telemedicine Development Services
Outside the US, similar regulations apply with regional adjustments: PHIPA and PIPEDA in Canada, GDPR plus the emerging European Health Data Space (EHDS) in the EU, the Data Protection Act 2018 plus DSPT in the UK, and the My Health Records Act in Australia. Each adds its own audit and data-residency requirements.
For US-bound EHR builds, the ONC Health IT Certification Program lists the technical and functional criteria certified EHR technology must meet, including the latest USCDI data classes and FHIR API requirements.
EHR Cost Breakdown by Module
A custom EHR is priced module by module, not as a single lump-sum figure. The breakdown below covers the modules a buyer typically scopes for a mid-size clinic build at $50–$80/hr. Each module has its own complexity drivers, so the actual figure for your project depends on which features you need within each one.
The table below shows typical effort and cost ranges for the six core modules in a mid-size custom EHR.
| Module | Effort | Cost at $50–$80/hr |
|---|---|---|
Patient records and EMR core | 250–600 h | $12,500–$48,000 |
Scheduling and appointment management | 150–400 h | $7,500–$32,000 |
E-prescriptions and pharmacy integration | 180–450 h | $9,000–$36,000 |
Billing, accounting, and payments | 200–500 h | $10,000–$40,000 |
Patient portal and mobile apps | 350–900 h | $17,500–$72,000 |
Reporting and analytics | 100–350 h | $5,000–$28,000 |
Core modules total | 1,230–3,200 h | $61,500–$256,000 |
Methodology: Effort ranges drawn from Cleveroad’s healthcare delivery records on custom EHR and clinic management builds between 2023 and 2025.
Patient records and EMR core
The foundational module: patient profiles, clinical notes, SOAP notes, and the underlying data model. Data model complexity is the main driver. A clinic capturing structured notes against a coded problem list runs higher than one capturing free-text notes alone.
- Effort: 250–600 h, cost: $12,500–$48,000.
Scheduling and appointment management
Real-time scheduling, provider calendars, automated reminders, and patient self-booking. Multi-location and telehealth booking push the cost up because each adds rules for availability, room or device assignment, and time-zone handling.
- Effort: 150–400 h, cost: $7,500–$32,000.
E-prescriptions and pharmacy integration
Cost is set largely by the third-party service. DoseSpot and Surescripts each have their own integration model, certification process, and per-transaction fees. The build includes drug interaction checks, allergy verification, and pharmacy routing.
- Effort: 180–450 h, cost: $9,000–$36,000.
Billing, accounting, and payments
Claims management, online patient payments, insurer data exchange, and reporting. Practice-management and clearinghouse integration is the variable that moves the cost most. A clinic billing five insurers through one clearinghouse runs at the low end; a multi-state practice billing through multiple clearinghouses sits at the top.
- Effort: 200–500 h, cost: $10,000–$40,000.
Patient portal and mobile apps
Web plus iOS plus Android, with appointment booking, secure messaging, results viewing, and intake forms. A web-only portal or a cross-platform Flutter build (as in our rehab clinic project) runs roughly $12,000–$20,000. Going native iOS plus native Android on top of web pushes the figure significantly higher.
- Effort: 350–900 h, cost: $17,500–$72,000.
Reporting and analytics
At the low end, internal and compliance reporting that pulls from your data tables. At the high end, custom dashboards, predictive analytics, and population health views. Most mid-size clinics start at the low end and expand the reporting layer in a second project phase.
- Effort: 100–350 h, cost: $5,000–$28,000.
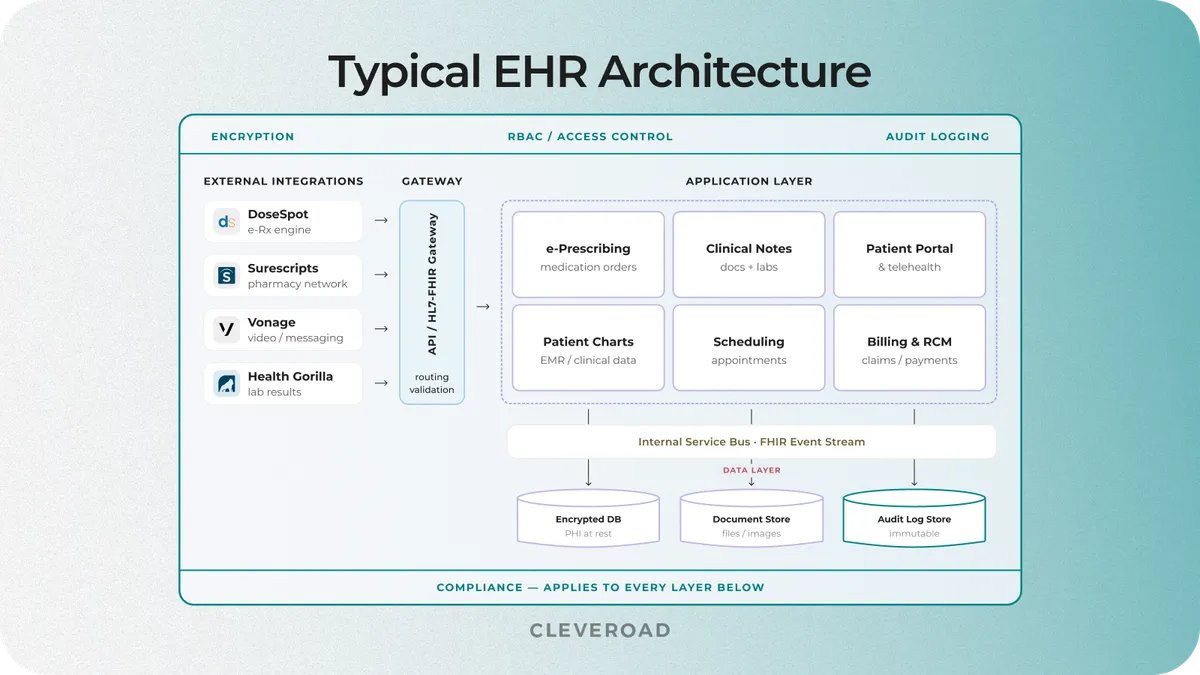
EHR architecture scheme
Why the Module Total Isn't Your Final Number
The number in the module table above is the development figure. The number on your invoice will be roughly double. Five cost lines sit around the build, and they are the difference between a defensible budget and a project that runs out of money in month seven.
Discovery and solution design
Discovery and solution design runs $4,000–$16,000 (80–200 h). This is the structured pre-build phase where the business analyst and Solution Architect map your clinic's workflow, lock the feature list, design the integration plan, and identify the compliance work.
A focused build with clear requirements lands at the low end. A clinic running on four disconnected SaaS tools that wants them unified needs deeper Discovery, which pushes the figure up. Skipping this phase is the single most expensive decision in an EHR project: without it, the rest of the estimate is based on assumptions, and mid-project change orders typically cost more than the entire Discovery budget would have.
Data migration
Data migration runs $5,000–$40,000 (100–500 h). The spread is driven almost entirely by the volume and quality of your existing records.
A SaaS-to-SaaS migration with clean structured data sits at the low end. Paper charts and handwritten notes scattered across legacy spreadsheets push the line toward the ceiling. The Hidden Costs section later in this article covers what tends to go wrong here and the buffer you should add to this line.
Compliance engineering
Compliance engineering runs $14,500–$60,000. The work happens across the build, not as a separate phase after development.
It covers audit logging in EMR core, encryption in the data layer, role-based access in scheduling, and BAA workflows in vendor integration. The itemized breakdown in the Compliance Scope section earlier in this article shows where each dollar goes. The high end hits when you need ONC certification readiness or a third-party security audit before launch.
Quality assurance
QA runs at 15–25% of total development effort. The 15% baseline covers a typical clinic build with limited integration.
The 25% ceiling hits when the project includes multi-system integration, regulated data flows, telehealth video, and the device and network test cycles those add on top of standard functional and security testing. QA hours are part of the engineering team's work, not a separate billable line bolted on at the end.
Project management
Project management runs 10–15% of development effort. This covers sprint planning, stakeholder communication, risk tracking, and the demo cycles that catch scope misalignment before it becomes rework.
Builds that cut PM to save money almost always pay for it through scope creep later in the project. The 10% baseline is needed even for the smallest serious EHR build; the 15% ceiling applies to multi-vendor or multi-location rollouts where coordination becomes its own job.
All-in for a mid-size custom build typically lands at $110,000–$450,000+. The $60,000–$255,000 figure cited in the module breakdown is core development only. The table below shows both figures side by side so you can see which one belongs in your budget meeting.
| Aspect | Core development only | All-in mid-size build |
|---|---|---|
Cost range | $61,500–$256,000 | $110,000–$450,000+ |
What's included | Six core modules built and tested | Modules + Discovery + migration + HIPAA + QA + PM |
What it represents | The figure most agencies quote in marketing | What the project actually costs to launch |
Methodology: All-in range derived from Cleveroad's mid-size EHR delivery records, adding the five cross-cutting lines above to the module total. Final figures depend on integration count, data migration scope, and compliance posture; confirm with a Solution Architect for project-specific scoping.
The Hidden Costs That Break EHR Budgets
The costs that overrun EHR budgets are rarely in the initial quote. They surface during migration, in the first months after go-live, and across the five-year maintenance window. Knowing where they sit lets you build a realistic buffer instead of running into them mid-project.
Data migration from legacy and paper records
Migration runs $5,000–$40,000 (100–500 h), and the spread is almost entirely driven by data volume and data quality. Clean structured data from a previous EHR migrates predictably. Paper charts, handwritten notes, and data spread across legacy spreadsheets do not.
Add a 20–30% buffer on this line when you scope it. In our rehab clinic project, the migration from the previous SaaS EMR included structured records plus partial paper archives, executed under HIPAA-compliant transfer protocols and full audit logging.
When migration involves legacy systems older than five years, opt for our legacy software modernization services that cover the assessment, transformation, and validation
Post-go-live productivity drop
Staff throughput drops 20–50% for the first 1–3 months after go-live. For a 20-person clinic, that loss often exceeds the entire direct training budget once you account for delayed billing, longer visit times, and rework.
Direct training cost itself runs $1,000–$5,000 per staff member, depending on whether you run classroom sessions, peer-trainer programs, or vendor-led shadowing. The productivity dip is the more expensive line, and it almost never appears in the original quote.
Integration rework and API surprises
Third-party APIs frequently look more mature in documentation than they are in production. The rework needed when a documented endpoint behaves differently, when sandbox data does not reflect live data shape, or when rate limits cap a feature you scoped — none of this gets quoted in advance.
In our healthcare builds, we set aside a contingency of 10–15% on integration work specifically to absorb this. Smaller buffers tend to leak into other lines and force a mid-project change order.
Ongoing maintenance and compliance updates
After go-live, plan for $1,500–$3,000 per physician per year for a SaaS-style maintenance contract, or 15–25% of build cost per year for a custom system. Compliance updates run continuously: HIPAA enforcement priorities shift, integration partners deprecate API versions, and audit cycles repeat on a fixed schedule.
Across a five-year window, maintenance is typically the largest single line in total cost of ownership for a custom EHR. Clinics that budget for build cost alone are usually surprised by year two.
Alex Penzov
CTO at Cleveroad
The line that breaks most EHR budgets is not in the build estimate at all. It is the productivity dip in the three months after go-live, where every clinical workflow runs more slowly until staff adapts. We tell clients to budget for that as if it were a fifth core module.

Off-the-Shelf vs. Custom EHR: The 5-Year Cost Comparison
The build-versus-buy decision is rarely close in year one and often flips by year five. Below is illustrative math for a 15-provider mid-size clinic on both paths, with the breakeven year called out.
Illustrative five-year total cost of ownership, 15-provider mid-size clinic:
- Off-the-shelf SaaS: licensing 15 × $300/month × 60 months = $270,000, plus setup, migration, and training of roughly $30,000, for about $300,000. Payments continue past year 5.
- Custom built EHR: roughly $150,000–$180,000 to build, plus maintenance of about $24,000/year × 5 = $120,000, for about $270,000–$300,000. The cost curve flattens after year 5, and the clinic owns the system.
- Breakeven lands around year 4–5; custom pulls ahead after that.
The chart below visualizes the two cost curves over the five-year window so you can see where breakeven happens for a clinic of this size.
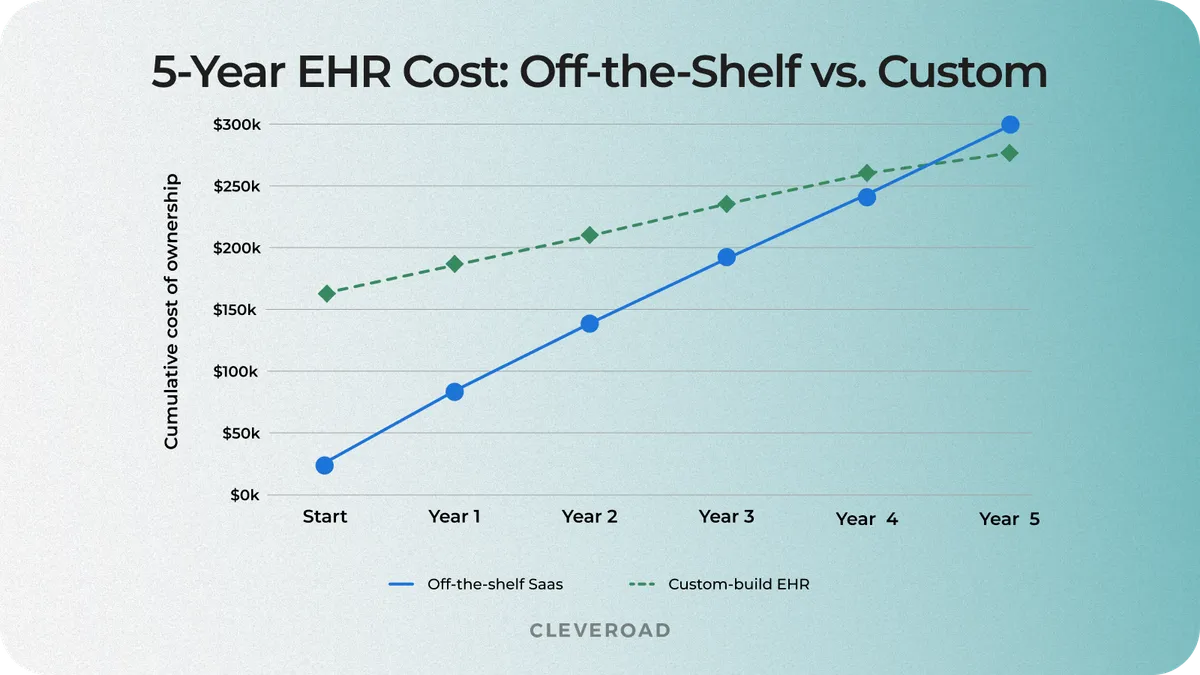
Five-year total cost of ownership: SaaS vs. custom EHR for a 15-provider clinic, with cumulative cost on the Y-axis and years 1–5 on the X-axis
When off-the-shelf is the cheaper choice
Small practices, standard workflows, no integration needs, and a fast launch — these are the cases where SaaS wins on cost and time. A solo practitioner who needs scheduling, billing, and basic notes can typically launch on a SaaS plan in under 30 days and stays cheaper than custom for the full life of the practice.
For many small clinics, the honest answer is buy, not build. Saying so directly saves the buyer six weeks of vendor calls.
When custom development pays back
Custom development pays back when one or more of these is true: you are paying for SaaS features you do not use, you run multiple disconnected systems that need consolidation, your integration needs exceed what the SaaS API supports, or your clinical workflow does not map cleanly to off-the-shelf software.
We’ll show you an example of when a custom solution fitted better based on our own experience. The case below shows how this played out for one of our customers, a US-based rehab clinic that was paying for unused SaaS features and juggling several disconnected systems.
Our client had been running on a per-provider SaaS EMR for several years. About 40% of the SaaS platform’s features sat unused, while staff juggled separate systems for scheduling, e-prescriptions, billing, and patient communication. The clinic needed a technical partner to:
- Replace the SaaS EMR with an owned platform that matches the clinic’s actual workflows
- Consolidate scheduling, e-prescriptions, billing, and patient apps under one system
- Meet HIPAA requirements end-to-end, with auditable data handling at every layer
- Migrate existing patient records from the previous EMR without service disruption
The Cleveroad team built a custom HIPAA-compliant platform on AWS that brought EMR core, scheduling, e-prescriptions, billing, and patient mobile apps into a single system. The stack used Node.js on the backend, React for the web admin, and Flutter for the iOS and Android patient apps. We integrated DoseSpot for e-prescribing and Vonage for the telehealth video layer, and secured the platform with AES-256 encryption, role-based access control, and a multi-AZ AWS deployment.
As a result, our client received a brand new clinic management system with EMR. The custom solution allowed them to drop annual software licensing cost roughly 40% after moving off the per-provider SaaS EMR to the owned system. Workflow-aligned functionality enabled the clinic to reduce administrative time on the affected workflows by 25%, returning several hours per staff member per week. Automated appointment reminders cut no-shows by 18%.
The screen below shows the clinic management interface combining scheduling, EMR access, and billing in a single view.
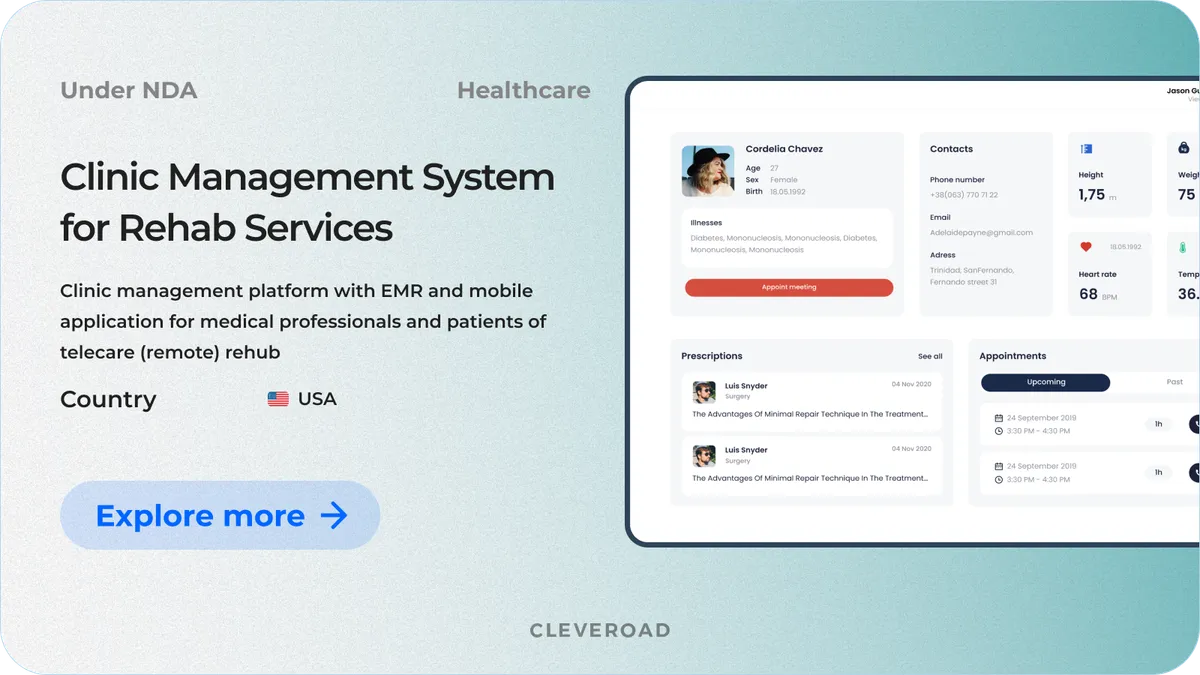
Clinic Management System developed by Cleveroad
- Explore the Clinic Management System case in more detail.
This kind of consolidation is how custom EHR pays back over a five-year window. The math works because the SaaS line stops accruing, and the new system replaces three or four disconnected tools.
How to Reduce EHR Implementation Costs Without Cutting Corners
Cutting the right things at the right time keeps the total down without compromising clinical workflow. Below are four practical levers that move the budget without leaving you with a half-built system.
Match the deployment model to your infrastructure
Decide between cloud and on-premises based on your internal IT capacity, not sticker price alone. A clinic with no dedicated IT team that picks on-premise inherits $50,000–$200,000 in avoidable upfront cost, plus the recurring overhead of running hardware with staff who are not equipped to maintain it. Cloud is usually the cheaper choice once you factor in the people cost of running the infrastructure.
Scope data migration before signing a contract
Assessing data volume and data quality before the contract is signed can move the migration line by tens of thousands of dollars and prevent mid-project change orders. Run a migration audit during Discovery: count the records, sample data quality, and identify which legacy systems will resist export. A 100-hour migration estimate built on bad assumptions can become a 500-hour migration in practice.
Roll out in phases, not all at once
A phased rollout limits the 20–50% productivity dip to one team or location at a time, rather than spreading it across the whole clinic in a single quarter. Start with one department or one core module, stabilize, then add the next. The total project duration is longer, but cash flow and revenue impact remain manageable.
Prioritize modules by clinical value
Build the revenue and care-critical modules first: EMR core, scheduling, and billing. Defer reporting, analytics, and secondary apps to a second phase. Deferring secondary modules can postpone 20–35% of the build cost into a later budget cycle while still launching the system on time.
How Cleveroad Can Help You Implement an EHR
Cleveroad is a custom software development company with 15+ years of experience building healthcare solutions for clinics, hospitals, and digital health startups. Our team includes 280+ in-house engineers and a 2,100-specialist external talent network, working across offices and R&D centers in Estonia, Poland, Ukraine, the US, and Norway.
For EHR projects specifically, we cover the full delivery cycle: business analysis, HIPAA-compliant architecture, custom development, third-party integration, and post-launch support. We hold ISO 9001 for quality management and ISO 27001 for information security, and we are an AWS Select Tier Partner, which matters for cloud-hosted EHR deployments.
What clinics get from working with us:
- HIPAA-compliant builds with audit logging, encryption, and role-based access designed in from the start, not added at the end
- Integration experience with DoseSpot, Surescripts, HL7/FHIR-based lab feeds, billing clearinghouses, and telehealth providers
- Four cooperation models matched to project scope and your in-house capacity: Dedicated Team, Staff Augmentation, Custom Development, and AI-Assisted Development team for rapid delivery
- A multi-level QA process covering functionality, integrations, performance, and security
- Post-launch maintenance and compliance update support across the five-year ownership window
How Cleveroad estimates EHR cost
Most agencies hand you one number. We produce two rough estimates and one detailed estimate at different points in the project, so the figure tightens as the scope clarifies.
- The first rough estimate comes after the Solution Design Workshop, based on a high-level scope and our delivery experience from comparable EHR projects. Each rough estimate is delivered in three scenarios: optimistic, realistic, and pessimistic, so you can decide whether to include every planned feature or focus on essentials within budget.
- The second rough estimate comes after the Discovery Phase, once detailed requirements, integration plans, and architecture decisions are in place. It sharpens the first estimate against the now-confirmed scope.
- The detailed estimate is produced during active development, sprint by sprint, by the business analyst and tech lead. This is the precise figure with 100% accuracy, and it lets you track spend against scope as features ship.
Get an EHR implementation cost estimate
Our Healthcare Solution Architects scope the project around your clinic’s modules and integrations, so you can plan the budget before committing to development.
Custom hospital EHR builds run $150,000–$1,000,000+, with multi-department enterprise rollouts going higher.
The average EHR implementation cost depends on facility size and whether you adopt SaaS or build custom. Small practices land at $3,000–$25,000 on SaaS or from $30,000 for a focused custom build. Mid-size clinics typically run $25,000–$150,000 on SaaS or $60,000–$255,000 for custom core development. These figures assume a development rate of $50–$80/hr; rates from US-based agencies typically run two to three times that, which pushes the custom figure proportionally.
It depends on the five-year window:
- Off-the-shelf wins in years 1–3, especially for small practices with standard workflows.
- Custom breaks even around year 4–5 for a 15-provider mid-size clinic.
- Custom pulls ahead after year 5, with the cost curve flattening while SaaS license fees continue.
For mid-size clinics paying for unused SaaS features or running disconnected systems, custom usually wins on a five-year view.
Plan for $1,500–$3,000 per physician per year on maintenance, plus continuous compliance updates as HIPAA priorities and integration partner APIs change.
A focused build for a small practice runs several months — typically 3–6 months for a SaaS adoption with limited integrations. A hospital implementation runs 12–24 months end-to-end, including multi-department integration testing and staff training.

Evgeniy Altynpara is a CTO and member of the Forbes Councils’ community of tech professionals. He is an expert in software development and technological entrepreneurship and has 10+years of experience in digital transformation consulting in Healthcare, FinTech, Supply Chain and Logistics
Give us your impressions about this article
Give us your impressions about this article